I borrow this old expression from Sesame Street to present a contrast that is indicative of the health care environment in the US, made all the more poignant by the fact that this is occurring in our nation's capital.
 This is United Medical Center, a safety net hospital serving one the poorest parts of the District of Columbia. The Washington Post reports that the District paid $12 million to Huron Healthcare to operate the hospital and make recommendations for its future.
This is United Medical Center, a safety net hospital serving one the poorest parts of the District of Columbia. The Washington Post reports that the District paid $12 million to Huron Healthcare to operate the hospital and make recommendations for its future.
Under its contract, Huron assumed management of United Medical Center in late March. It is undertaking a “strategic review” of the hospital’s operations and is expected to develop a proposal to help turn around the hospital in the coming weeks for the approval of the hospital’s board in July.
(By the way, I provided recommendations pro bono a few months ago. Remind me to raise my rates!)
That UMC is failing financially is a multifaceted problem, but it basically a result of the structure of compensation provided to safety net hospitals. The body politic in DC--including the US Congress and the current Administration--has failed to deal with the issue. The result is a degradation in the quality and availability of service to people in this neighborhood. As I have said:
The DC government and local constituencies will only solve UMC's problems when the federal government makes the proper commitment to providing the poor people in this part of the District with "a full-service hospital east of the Anacostia River."
Meanwhile, look what's happening a few miles away, as a result of the kind of federal commitment that can send tens of millions of dollars to wasteful clinical endeavors. This is MedStar Georgetown University Hospital:

This is Sibley Memorial Hospital, affiliated with Johns Hopkins Medicine:

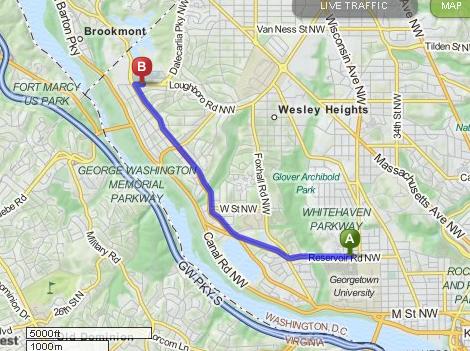
This is a map of their relative locations, about 3 miles apart:

The two hospitals have both just received permission from the District of Columbia to install proton beam radiation therapy machines, at a total cost of $153 million. The Post notes:
The decision has been closely followed by health experts because critics say it reflects a nationwide medical arms race, as hospitals scramble for dominance by investing millions of dollars in technology that has not been proven to be better than cheaper alternatives for some cancers.
Jenny Gold at NPR reported:
"Neither [Hopkins nor MedStar] should be building," says Dr. Ezekiel Emanuel, a former health care adviser to the Obama administration who is now at the University of Pennsylvania. "We don't have evidence that there's a need for them in terms of medical care. They're simply done to generate profits."
Meanwhile, another facility, the Maryland Proton Treatment Center, is already being built 40 miles away in downtown Baltimore.
The organization that is making this possible is CMS, which has set rates for use of proton beams for "normal" cancer therapy that far exceed their value compared to traditional forms of radiotherapy.
Dr. Emanuel was a key advisor to President Obama on health care issues. He and others in the administration have had years to fix this problem, but they have not. When I recently asked a high ranking CMS official why they didn't act to change this payment scheme, s/he answered, "I think you know the reason why." The reason why, obviously, was that political pressure from those who stand to benefit from the medical arms race have enough influence on the federal agencies to protect the status quo.
When we compare the outright waste of tens of millions of dollars on duplicate machines of unproven clinical effectiveness with the human suffering that results from the degradation of places like United Medical Center, we see political corruption of the highest order. I am not suggesting personal corruption, nor I am suggesting that either political party is solely responsible. I am suggesting corruption of political processes to protect the strong, big, and well connected at the expense of the poor and less powerful.
Under its contract, Huron assumed management of United Medical Center in late March. It is undertaking a “strategic review” of the hospital’s operations and is expected to develop a proposal to help turn around the hospital in the coming weeks for the approval of the hospital’s board in July.
(By the way, I provided recommendations pro bono a few months ago. Remind me to raise my rates!)
That UMC is failing financially is a multifaceted problem, but it basically a result of the structure of compensation provided to safety net hospitals. The body politic in DC--including the US Congress and the current Administration--has failed to deal with the issue. The result is a degradation in the quality and availability of service to people in this neighborhood. As I have said:
The DC government and local constituencies will only solve UMC's problems when the federal government makes the proper commitment to providing the poor people in this part of the District with "a full-service hospital east of the Anacostia River."
Meanwhile, look what's happening a few miles away, as a result of the kind of federal commitment that can send tens of millions of dollars to wasteful clinical endeavors. This is MedStar Georgetown University Hospital:
This is Sibley Memorial Hospital, affiliated with Johns Hopkins Medicine:
This is a map of their relative locations, about 3 miles apart:
The two hospitals have both just received permission from the District of Columbia to install proton beam radiation therapy machines, at a total cost of $153 million. The Post notes:
The decision has been closely followed by health experts because critics say it reflects a nationwide medical arms race, as hospitals scramble for dominance by investing millions of dollars in technology that has not been proven to be better than cheaper alternatives for some cancers.
Jenny Gold at NPR reported:
"Neither [Hopkins nor MedStar] should be building," says Dr. Ezekiel Emanuel, a former health care adviser to the Obama administration who is now at the University of Pennsylvania. "We don't have evidence that there's a need for them in terms of medical care. They're simply done to generate profits."
Meanwhile, another facility, the Maryland Proton Treatment Center, is already being built 40 miles away in downtown Baltimore.
The organization that is making this possible is CMS, which has set rates for use of proton beams for "normal" cancer therapy that far exceed their value compared to traditional forms of radiotherapy.
Dr. Emanuel was a key advisor to President Obama on health care issues. He and others in the administration have had years to fix this problem, but they have not. When I recently asked a high ranking CMS official why they didn't act to change this payment scheme, s/he answered, "I think you know the reason why." The reason why, obviously, was that political pressure from those who stand to benefit from the medical arms race have enough influence on the federal agencies to protect the status quo.
When we compare the outright waste of tens of millions of dollars on duplicate machines of unproven clinical effectiveness with the human suffering that results from the degradation of places like United Medical Center, we see political corruption of the highest order. I am not suggesting personal corruption, nor I am suggesting that either political party is solely responsible. I am suggesting corruption of political processes to protect the strong, big, and well connected at the expense of the poor and less powerful.